by Woodsbum
Seeing as how it is still elk season and I just ran across this, I felt compelled to include this article as today’s post.
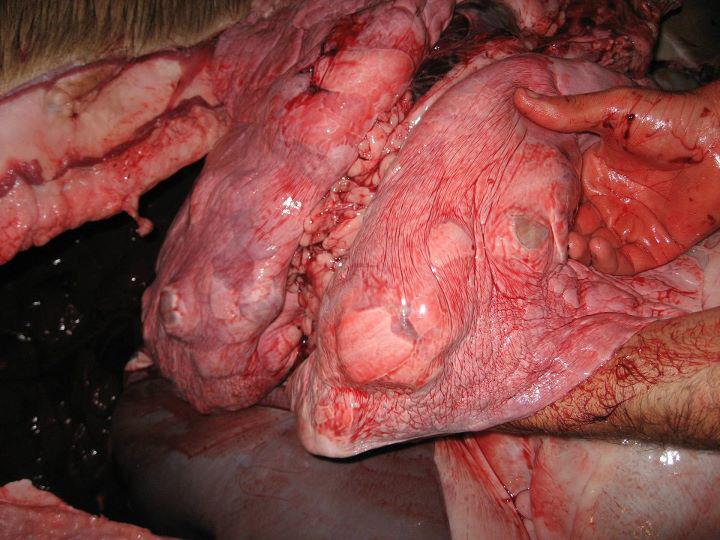
Echinococcosis hydatid cyst or cystic echninococcosis (CE) is a condition where a small tapeworm actually grows in the lungs, thus causing a cyst. The following article really explains it quite well, but the important point is that any time you run across these cysts in an animal’s lungs you should be extremely careful and assume that the meat is NOT fit for consumption.
Here is the article:
****************************************************************************
Background
Cystic echinococcosis (CE) is the larval cystic stage (called echinococcal cysts) of a small taeniid-type tapeworm (Echinococcus granulosus) that may cause illness in intermediate hosts, generally herbivorous animals and people who are infected accidentally. Ultrasonographic appearance of echinococcal cysts is seen in the image below.
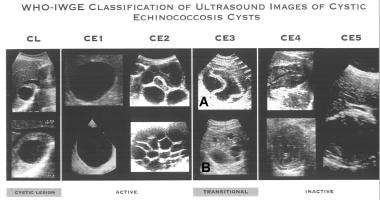 WHO Informal Working Group on Echinococcosis standardized ultrasound classification of echinococcal cysts. Image courtesy of World Health Organization (WHO).
WHO Informal Working Group on Echinococcosis standardized ultrasound classification of echinococcal cysts. Image courtesy of World Health Organization (WHO). Three other species are recognized within the genus Echinococcus, and they may also develop in the human host and cause various forms of echinococcosis (hydatidosis). E granulosus is discussed separately from the other 3 species, notably Echinococcus multilocularis, which causes alveolar echinococcosis, because of marked differences in epidemiology, clinical features, diagnosis, and treatment.
In the normal life cycle of Echinococcus species, adult tapeworms (3-6 mm long) inhabit the small intestine of carnivorous definitive hosts, such as dogs, coyotes, or wolves, and echinococcal cyst stages occur in herbivorous intermediate hosts, such as sheep, cattle, and goats. A number of other suitable intermediate hosts, such as camels, pigs, and horses, are involved in the life cycle in many parts of the world.
In the typical dog-sheep cycle, tapeworm eggs are passed in the feces of an infected dog and may subsequently be ingested by grazing sheep; they hatch into embryos in the intestine, penetrate the intestinal lining, and are then picked up and carried by blood throughout the body to major filtering organs (mainly liver and/or lungs). After the developing embryos localize in a specific organ or site, they transform and develop into larval echinococcal cysts in which numerous tiny tapeworm heads (called protoscolices) are produced via asexual reproduction.
These protoscolices are infective to dogs that may ingest viscera containing echinococcal cysts (with protoscolices inside), mainly because of the habit in endemic countries of feeding dogs viscera of home-slaughtered sheep or other livestock. Protoscolices attach to the dog’s intestinal lining and, in approximately 40-50 days, grow and develop into mature adult tapeworms, once again capable of producing infective eggs to be passed to the outside environment with the dog’s feces.
Because humans play the same role of intermediate hosts in the tapeworm life cycle as sheep, humans also become infected by ingesting tapeworm eggs passed from an infected carnivore. This occurs most frequently when individuals handle or contact infected dogs or other infected carnivores or inadvertently ingest food or drink contaminated with fecal material containing tapeworm eggs.
Pathophysiology
In primary echinococcosis, metacestodes develop from oncospheres after peroral infection with E granulosus eggs. In secondary echinococcosis, larval tissue proliferates after being spread from the primary site of the metacestode. This can occur by spontaneous trauma such as induced rupture or during medical interventions.
In primary echinococcosis, larval cysts may develop in every organ. Most patients (as many as 80%) have single-organ involvement and harbor a solitary cyst. Approximately two thirds of patients experience liver echinococcosis. The second most common organ involved is the lung.
In each anatomic site, cysts are surrounded by the periparasitic host tissue (pericyst), which encompasses the endocyst of larval origin. Inside the laminated layer, or hyaline membrane, the cyst is covered by a multipotential germinal layer, giving rise to the production of brood capsules and protoscolices. The central cavities of cysts of E granulosus are filled with clear fluid, numerous brood capsules, and protoscolices. In addition, daughter cysts of variable size are often detected. The growth rate of cysts is highly variable and may depend on strain differences. Estimates of the average increase of cyst diameter vary (approximately 1-1.5 cm/y).
The clinical features of cystic echinococcosis are highly variable. The spectrum of symptoms depends on the following:
-
Involved organs
-
Size of cysts and their sites within the affected organ or organs
-
Interaction between the expanding cysts and adjacent organ structures, particularly bile ducts and the vascular system of the liver
-
Complications caused by rupture of cysts
-
Bacterial infection of cysts and spread of protoscolices and larval material into bile ducts or blood vessels
-
Immunologic reactions such as asthma, anaphylaxis, or membranous nephropathy secondary to release of antigenic material
Epidemiology
Frequency
United States
Unfortunately, realistic national or international figures do not exist for total numbers of cases of cystic echinococcosis. The problem is that, until recently, the only basis for diagnosis was surgery, and few countries systematically reported cases. When they did report cases, uneven reporting occurred in different regions of countries. The groups most at risk of cystic echinococcosis are usually underserved by medical services.
However, the increasing use of mass screenings with ultrasonography in endemic countries is generating important epidemiological data. As different cyst stages have been classified according to their sonographic appearance, attempts are being made to match the cyst morphology with the natural history of the cyst. This is evident with the World Health Organization (WHO) standardized classification (see Imaging). At a community level, the relative proportions of cyst types can provide epidemiological information on disease transmission and help design effective control programs.[1]
In the United States, transmission of E granulosus in the dog-sheep cycle is known to occur most frequently in several western states, including California, Arizona, New Mexico, and Utah. In Arizona and New Mexico, cystic echinococcosis is known to occur in American Indians belonging to the Zuni, Navajo, and Santo Domingo tribes, whose members live in close proximity to their animals, kill many of their own animals each year, and generally have limited knowledge concerning the life cycle and transmissibility of the parasite. In the United States, Utah has had the highest number of surgical cases of those states involved, with approximately 45 cases from 1944-1994.
International
E granulosus is a cosmopolitan parasite, and endemic regions exist in each continent. Considerable public health problems occur in many areas, including countries of Central America and South America, Western and Southern/Southeastern Europe, the Middle East and North Africa, some sub-Saharan countries, Russia and adjacent countries, and China. Annual incidence rates of diagnosed human cases per 100,000 inhabitants vary widely, from less than 1 case per 100,000 to high levels. For example, rates in the indicated regions are as follows:
-
Greece – 13 cases per 100,000 persons
-
Rural regions of Uruguay – 75 cases per 100,000 persons
-
Rural regions of Argentina – 143 cases per 100,000 persons in Rio Negro province
-
Parts of Xinjiang province of China – 197 cases per 100,000 persons
-
Parts of the Turkana district of Kenya – 220 cases per 100,000 persons
Cystic echinococcosis causes not only illness but also productivity losses in human and agricultural animal population, and it can have large societal impacts on endemic areas. Research is being conducted to evaluate the burden of disease, including nonmonetary costs.
Mortality/Morbidity
Cystic echinococcosis is rarely fatal. Occasionally, deaths occur because of anaphylactic shock or cardiac tamponade in heart echinococcosis.[2]
Rare locations of the cyst (muscle, bone, brain, orbit) can cause dramatic and disabling symptoms (blindness, paralysis).[3, 4, 5, 6, 7, 8, 9, 10]
Race
No racial predilection exists.
Sex
In some endemic countries, females are affected more than males because their lifestyle habits and practices bring them into contact with the parasite.
Age
Individuals of all ages are affected. In some endemic countries, children have higher infection rates because they are most likely to play with dogs.
History
Months or years may pass before an individual exhibits any signs or symptoms of infection with the cystic larval stages.
During the natural course of infection, the fate of E granulosus cysts is variable. Some cysts may grow to a certain size and then persist without noticeable change for many years. Other cysts may rupture spontaneously or collapse and completely disappear.
Spontaneous or traumatic cyst rupture and spillage of viable parasitic tissue during interventional procedures may result in secondary echinococcosis. Cysts may rupture into the peritoneal or pleural cavity, the pericardium, the bile ducts, the gastrointestinal tract, or even blood vessels, leading to extraordinary manifestations and severe complications.
Spontaneous cure of cystic echinococcosis is possible.
After a variable incubation period, infections may become symptomatic if cysts are growing and exerting pressure on adjacent tissue and inducing other pathologic findings.
Sudden symptomatology is usually due to spontaneous or traumatic cyst rupture.
Usually, cysts do not induce clinical symptoms before they have reached a size sufficient to exert pressure on adjacent organs.
Physical
The presentation of human echinococcosis is protean. Patients come to the clinician’s attention for different reasons, such as when a large cyst has some mechanical effect on organ function or rupture of a cyst causes acute hypersensitivity reactions. The cyst may also be discovered accidentally during radiographic examination, body scanning, surgery, or for other clinical reasons.[11]
Common chief symptoms are upper abdominal discomfort and pain, poor appetite, and a self-diagnosed mass in the abdomen. Physical findings are hepatomegaly, a palpable mass if on the surface of the liver or other organs, and abdominal distention. If cysts in the lung rupture into the bronchi, intense cough may develop, followed by vomiting of hydatid material and cystic membranes.[12]
Liver findings may include the following:
-
Hepatomegaly
-
Jaundice
-
Biliary colic–like symptoms
-
Cholangitis
-
Pancreatitis
-
Liver abscess
-
Portal hypertension
-
Ascites
-
Inferior vena cava compression or thrombosis
-
Budd-Chiari syndrome
-
Cyst rupture, peritoneal spread, and peritonitis
-
Hemobilia
-
Biliary fistula to skin, bronchial system, or gastrointestinal tract
Lung findings may include the following:
Heart findings may include the following:
-
Tumor
-
Pericardial effusion
-
Embolism
Breast masses may be found (must be differentiated from neoplasms).[11]
Spine masses with neurologic symptoms may be found.
Brain masses with neurologic symptoms may be found.

CE
****************************************************************************
So there you have it. If you see any animal lungs that have cysts that resemble the picture above you should immediately assume that the meat is tainted and not fit for consumption. Make sure to take a picture of the infected animal’s lungs and you can forward it to any number of organizations that are monitoring this condition.
Again, there is much speculation as to why this is occurring, but much finger pointing is direction towards the wolves that were reintroduced to the Western United States. From what I have read, the current species of wolf that was introduced is actually a different species than what originally lived here. That also accounts for the tremendous increase of wolf numbers over the last several years.
No matter what side of the wolf debate you are on or even if the wolf was the cause of this tapeworm that is infecting the herbivores of the Western States it is 100% fact that this is a problem that needs to be researched.
Be careful out there!!